Bearing the Burden
Fresno’s mothers of color are suffering, and the city wants to help.
Why is that so hard?
Fresno’s mothers of color are suffering, and the city wants to help.
Why is that so hard?
When baby Rodrigo was born, he didn’t make a sound. Lucy had been in the hospital for a week since she first showed signs of labor. That week brought her just past the 23 week mark of her pregnancy. That’s when doctors would agree to medically intervene to keep her baby alive.
Lucy lay on her side. There was just quiet. No baby cry, no activity. The doctor said,
“He's been born in his sac. Please don't push. I need your placenta there because the NICU team is still not here. So just don't push. I'll let you know when to push. It must have taken them like three to five minutes. But it was eternal.”
When the team arrived, they whisked the baby away. A half hour passed. She remembers a nurse practitioner came to Lucy’s side and told her,
“Your son is alive but we can't guarantee anything. His chances of survival are about 20 percent. And if he survives we want you to know that he most likely won't breathe on his own. He will never walk. He will never speak. He will be a vegetable.”
Lucy didn’t have the birth she wanted. Neither did nearly eight thousand women in America this week. Doctors call these cases -- preterm birth, low birthweight babies, and infant mortality -- adverse birth outcomes. But a woman’s account of her “outcome” tells a story far longer than the course of her pregnancy.
As the nurse practitioner listed the statistics of terrible things that would probably happen to Rodrigo, Lucy piled each sentence on her own shoulders. She must have done something wrong. She was to blame. The dogma of “personal responsibility” bears a lot of weight. But how a pregnancy turns out is more than the product of a woman’s decisions. Responsibility stretches into the distant past, and far beyond the skin she lives in. Into medical examination rooms years before conception. Into city planning offices and budget meetings.
Public health workers say that pregnancy outcomes are a barometer of the health of a community, and a predictor of the health of a community’s next generation. Well-intended efforts haven’t solved the problem that outcomes vary, sometimes dramatically, by race. Birth statistics ebb and flow, but never reach equality. Now, public health is looking at the problem through a new lens.
Fresno County’s rates of preterm birth, babies born before 37 weeks, are among the highest in the country. In one southwest Fresno ZIP, the rate is 12 percent. And for black women living in that ZIP, it’s 21 percent. For white women in a wealthier north Fresno neighborhood, it’s five percent.
The problem of adverse birth outcomes is viewed as so severe by Fresno civic leaders that they’ve joined with a coalition of researchers, to address it. The city is one of six in the world to be included in The Preterm Birth Initiative, a 10-year, $100 million research effort backed by the University of California at San Francisco and private funding.
John Capitman, director of the Central Valley Health Policy Institute, was one of the early developers and leaders of the initiative. He doesn't believe that the commonly cited risk factors - poverty, drug use, and homelessness - get to the heart of birth-related health disparities. The Centers for Disease Control and Prevention lists “black race” as one of its risk factors. But Capitman and his colleagues believe that it’s racism, not race, that should be recognized as a risk factor.
“We're talking about the impacts of racism and poverty and how our public systems do or do not mediate those impacts on people's health status... In a way that's a litany of the impacts of of racism and poverty on people's lives. That in turn both produce greater risk of disease and less access to health care.”
- Dr. John Capitman
In Fresno, racism and concentrated poverty are inextricably linked by a long history of segregation. Physical segregation and housing segregation was accompanied by a gulf in quality of care and access to services.

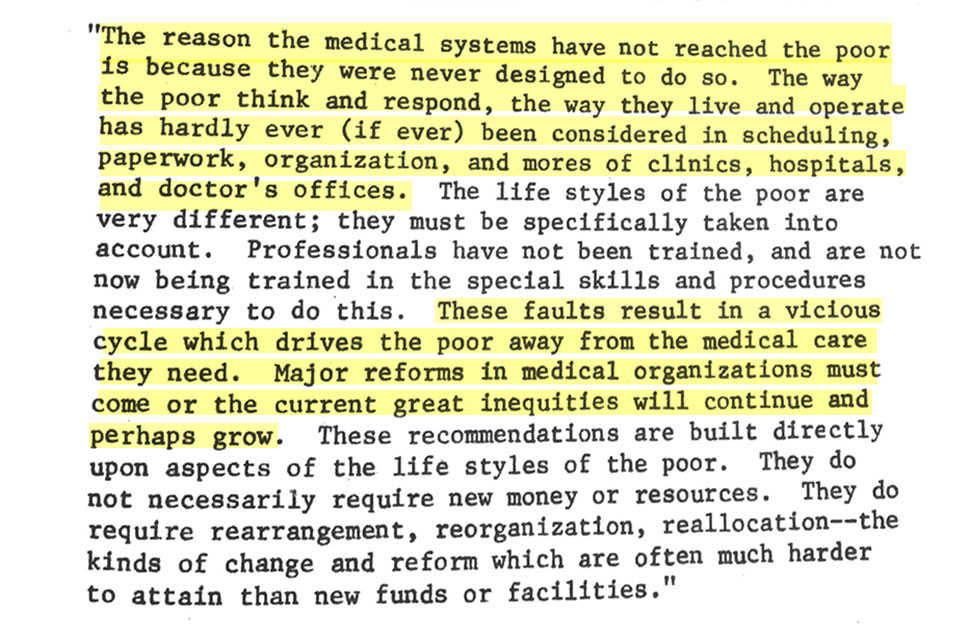
Inequality’s influence on health has been formally recognized in Fresno before. In 1974, the Fresno Department of Public Health laid out a vision for reorganizing the system, wielding excerpts from a national journal article called “Medical Ghettos:”
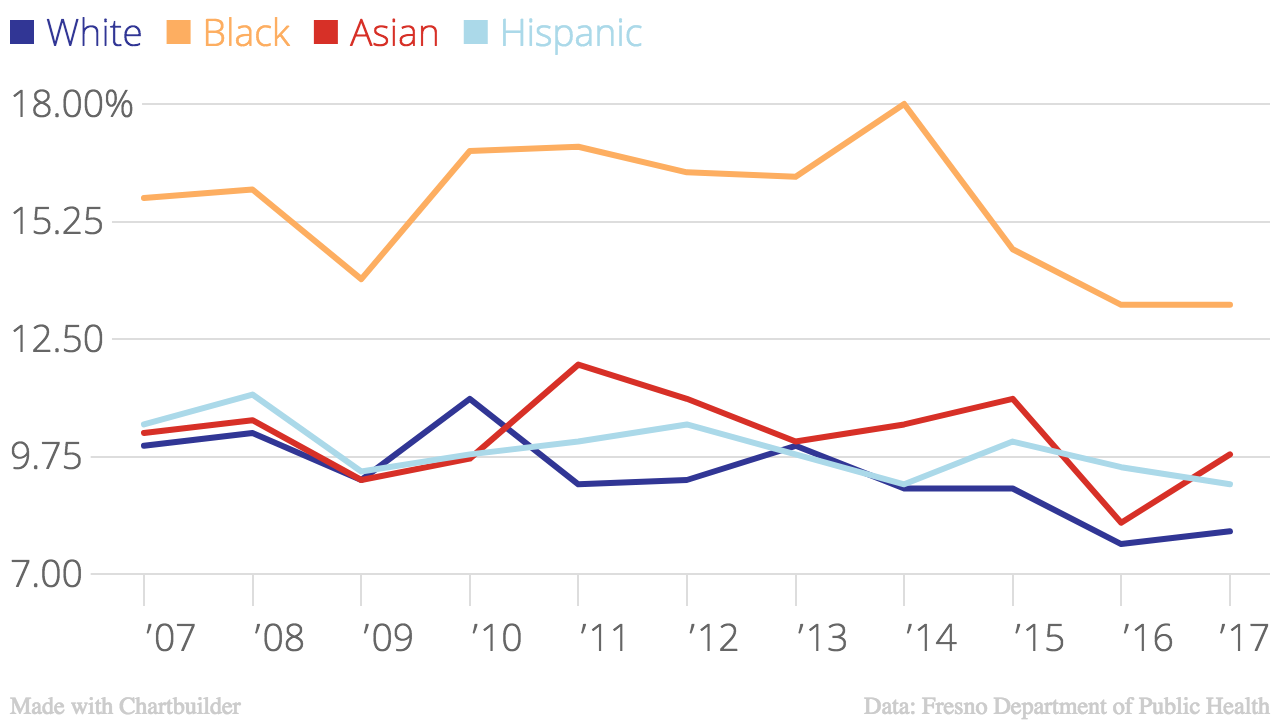
For half a century, there’s been talk of better public health services for the entire community. There have been periods of significant improvement. Between 1992 and 2001, the county's black infant mortality rate decreased from 37.1 to 11.4 per 1,000 births. But there has been backsliding. The black infant mortality rate increased 87 percent between 2007 and 2014, from 14.5 to 27.3 per 1,000 births. In part because of this regression, the progressive public health conversation is shifting again, from addressing poverty to addressing systemic racism.
The shift is particularly relevant in Fresno, where the population is nearly 60 percent hispanic and its residents speak 62 languages. It’s also where race is a strong determinant of how a woman’s birth will play out.
Despite the diversity of patients in Fresno, its public health workers recognize that the healthcare system is not a welcoming environment for all. That’s what has made it difficult for Shanae Fuller, an African American mother of two, to have faith that doctors care about what she thinks and feels. Based on the color of her skin, she says, she gets one of two messages: “How do you know that?” and “Wouldn’t you like to know?”
Rose Mary Rahn is the division manager of Public Health Nursing in Fresno’s Department of Public Health. “How do we tackle that the health care providers are not being culturally competent?” she asks. “I’ve heard that complaint numerous times.” Cultural competence is a workplace euphemism for non-racist service, for providing services that “meet the social, cultural, and linguistic needs of patients.”
In Fresno, and around the country, researchers have uncovered inequities in medical treatment. There’s a different threshold for pain treatment for minorities and whites. The findings of one study show that in appendicitis cases, black children are less likely than white to receive pain medication. Pregnant women are also treated unequally. A national survey found that only one in three hispanic women with diabetes is tested for high blood sugar after birth. That’s compared to two in three black and white women. More black and hispanic women met their delivery doctor for the very first time during their birth than white women.
These statistics contaminated the sterile hospital air when Shanae Fuller’s son spent months in the NICU. Her faith in the interests of her son’s doctors weakened over time. She felt that doctors wanted to shuttle him out of the NICU by any hasty procedures necessary. In one case, her son’s doctor all but began a surgical procedure that Shanae wholeheartedly disagreed with. She found herself grasping at every scrap of terminology she could remember in order to push back against her doctor’s recommendations. She wondered if the doctor’s resistance had to do with her race.
First 5 Fresno, a public organization that invests in direct services for young children and their families, conducted a survey to measure how moms were feeling during their perinatal period, the period of time just before, during, and after birth. The study asked whether a patient’s doctors or their child’s pediatrician gave them the time and “cultural sensitivity” to discuss their issues. Forty-four percent of moms said no. Shanae is a mother who might have said no, too. Hear her story here:
“He couldn't explain to us, in a normal sense, what it was. And from then on, they told us that he wasn't going to make it."
Over the past five years, only 10 complaints were filed against OB/GYNs in Fresno. But that may not be a reflection of a system free of complaints.
Black Infant Health is a regional public health program that works directly with pregnant African-American women and new moms. Fanta Nelson, the coordinator of the program, said that many of her clients don’t complain because they’re scared of retaliation during their hospital stay. For the health of themselves and their babies, she says, they stay quiet. Others are simply resigned to the status quo. “Out of sight out of mind,” she says. “It happened to me. It's not the first time.”
Joe Prado, division manager of community health for the Department of Public Health, says that for all providers of care to become truly “culturally competent,” it would require a system-wide approach to training. He likened such a change to the adoption of HIPPA. “Whenever you want to institute something of that magnitude it's going to have to be legislatively driven,” he says. Shanae never considered filing a complaint for the cultural incompetence she experienced.
There’s a cost to adverse birth outcomes, economically, on communities and families. The Center for Disease Control estimates that preterm births cost the United States $26 billion per year. In Fresno County, care for preterm babies costs the health system about $78 million per year. Lucy Gomez was on private insurance when she gave birth to Rodrigo at 23 weeks. The cost of her son’s five-month NICU stay totalled nearly $2 million.
Lucy had the stability of private insurance for those months, but she felt uncertainty about the months and years to come. Not just about her family’s savings, but about Rodrigo’s strength. Preterm babies are more likely to develop health complications in the future, and complications from preterm birth is the leading cause of death for children under five.
There are other costs to the mother. Invisible, long-lasting ones. Researchers are trying to get to the bottom of the causes of preterm birth, honing in on racism as a factor. But the factors that might lead to an adverse birth don’t fade away after nine months. And those factors are compounded when a difficult birth actually happens.
Simply having a baby in the neonatal intensive care unit (NICU) of a hospital puts parents at risk for PTSD. For every three babies warmed by an incubator, one mom meets the criteria for PTSD at their infant’s NICU admission. That experience has lasting consequences. While 10-15% of mothers of healthy babies meet the criteria for postpartum depression, one study shows that diagnosis can be made for at least 50% of mothers of babies in the NICU.
The stress can start immediately. Just after Shanae’s baby was born, she watched a helicopter fly him for emergency surgery 15 miles away. At the same moment, her mother and boyfriend drove away. She was abruptly alone, left to steep in her own fears of what would happen to her baby next.
Stress from the NICU can be unrelenting, lingering between visits and after discharge. Five months after her son’s birth, Lucy’s family prepared to take Rodrigo home from the NICU. Home, without the guarantee of a medical staff’s watchful eye, without the beeping surveillance of Rodrigo’s every bodily function. As much as Rodrigo transformed over the course of his NICU stay, Lucy had changed as well. Then, Lucy got a piece of news that altered her course even further. Listen to Lucy’s story here:
“You ask yourself what did I do wrong... When you try to put grief aside it will come back. With a vengeance. And that's exactly what happened to me."
A mother’s mental health is connected to how her child develops, adapts, and learns. Dr. Cassandra Joubert is director of the Central California Children's Institute, and has studied the mental health of mothers and infants in Fresno for 10 years. She says that the quality of the mother-infant relationship in the earliest part of a child’s life is a strong predictor of childhood wellbeing.
“If a mom is depressed, she's not able to give her child, through interaction and through a nurturing relationship, what that child needs for healthy brain development. And without that healthy brain development in the first few years of life, by the time you're three you're already at a disadvantage.”
-Dr. Cassandra Joubert
And yet, only half of the city’s OB/GYN providers said that they formally screen moms for depression. And slightly more than half of all perinatal medical providers said they don’t know enough about maternal depression. Three quarters of providers, including behavioral health providers, said they weren’t trained to deal with the mood disorders that go along with the pregnancy period.
A bill before California’s legislature would require providers to screen for anxiety and mood disorders during prenatal, postpartum, and well child visits. The legislation actually makes it a crime for providers to not screen their patients.
But in a Fresno survey, most providers said they didn’t screen because they didn’t know where to refer for maternal depression. The Department of Public Health acknowledges that there might not be enough mental health providers to refer patients to. But Rose Mary Rahn, the manager of Fresno’s public health nursing says the problem might be more complicated. “I know mental health tries to serve everybody, but sometimes women don't want the services,” she says. “I mean there's a whole gamut of things.” But experts like Joubert and Capitman believe that women aren’t being served now, and point to alternative approaches.
Joubert advocates moving away from the one-on-one clinical model, and towards a more efficient one that actually defers to the comfort of patients. Find a few mental health professionals who want to specifically treat maternal depression, she suggests. Those licensed clinicians would provide care in group settings that make sense for the community.
She points, for example, to church. “We have learned in our work that in Fresno that African-Americans feel more comfortable and supported in faith environments,” she explains. So bringing mental health professionals to church might be a good approach.
Culturally-specific, targeted, and alternative approaches to health care do exist in the system already. One of those is Black Infant Health, a state-wide public health program for African-American moms. It’s designed to address the needs of the African-American population, often in group settings.
La’Shawn Gaines has struggled with depression for over a decade. It was only during her pregnancy, when she was screened, that she heard that her suffering had a name. And still, it took years of more pain before she got help. Hear her story here:
"My eight year old, sometimes she comes in like, 'You're not having a good day today, huh, Mama?'
...Hopefully one day it will be over with."
A targeted, group approach satisfies some of a mother’s deepest desires. “That sense of of just not being an outlier. That sense of just being normal. That's what all of us seek,” says Joubert. “So many women report that they don’t know of other women who are going through what they’re going through.” She says that for too long, public health has underestimated the importance of social support.
That same supportive group approach to mental health care could be applied to a range of medical needs, like prenatal visits. La’Shawn felt so distrustful of the nurse practitioner who saw her during her prenatal appointment that she didn’t go back.
The Preterm Birth Initiative is trying the group approach to care with a demonstration project called Glow!. It’s a trial run, funded by private donors. Its participants get their care through group prenatal visits, and get childcare and transportation assistance for those visits. A 2007 study in the journal Obstetrics and Gynecology showed a a 33 percent reduction in preterm births for mothers who get their care through group visits. If Glow! proves successful, it could provide a model for replication.
These initiatives require investment and the Fresno Department of Public Health says that targeted programs are often the first thing to go. “In the public health basket, when we lose the money everybody loses,” says Joe Prado. “Everybody suffers.”
In Fresno’s recent history, changes in spending on maternal and infant care had serious consequences. Black Infant Health, the public health program approach to healthcare, social support, and education seems to go along with positive change: in the ten years after it was established, the county's black infant mortality rate decreased by two thirds. But cuts to its funding seemed to change that. In 2007, Black Infant Health had 11 employees and a $1.3 million budget. After the economic recession, in 2010, the organization had two employees and a $250,000 budget. In that span of time, the county’s black infant mortality rate more than doubled, to 27.3. That’s nearly three times the statewide average that year. And in 2011, there were fewer high-risk women enrolled in prevention programs.
Of course, lots of factors go into the fluctuation of preterm birth and infant mortality rates. But what happened in Fresno suggests an association between funding reductions for services like BIH and and infant mortality. But population-specific programs are often the first to go. Joubert says that tailored support shouldn’t be seen as an addition to basic care; it is basic care.
“To support a black infant health program is an acknowledgment of that reality and people struggle with that... We suffer as a nation if we fail to acknowledge those disparities. There's all of this push for we need evidence-based approaches. Well what good is evidence if you won't use it?”
-Dr. Cassandra Joubert
Fresno Health officials recognize the limitations and failures of the current healthcare structure. Department reports consistently argue that the healthcare system needs to work for the people they serve, through programs that foster social support. Whether the community sustains its investment in those programs will be a test of whether the public health lens has truly shifted.
What’s known without question is that an investment in mothers delivers returns. After Lucy lost her baby in 2017, she had good medical care to recover physically, and found a counselor to help her recover mentally. She and her husband tried to get pregnant again, and she did. She’d learned a lot over the years. She started interventions at 8 weeks. On April 21, Lucy went into labor again. This time, the labor was early, but just by a few weeks. She delivered Francisco Xavier, a healthy five pound, five ounce boy by c-section. When she heard his cry, she says, it was the most beautiful sound on earth.

